Ductal Carcinoma In Situ (DCIS)


What is ductal carcinoma in situ (DCIS)?
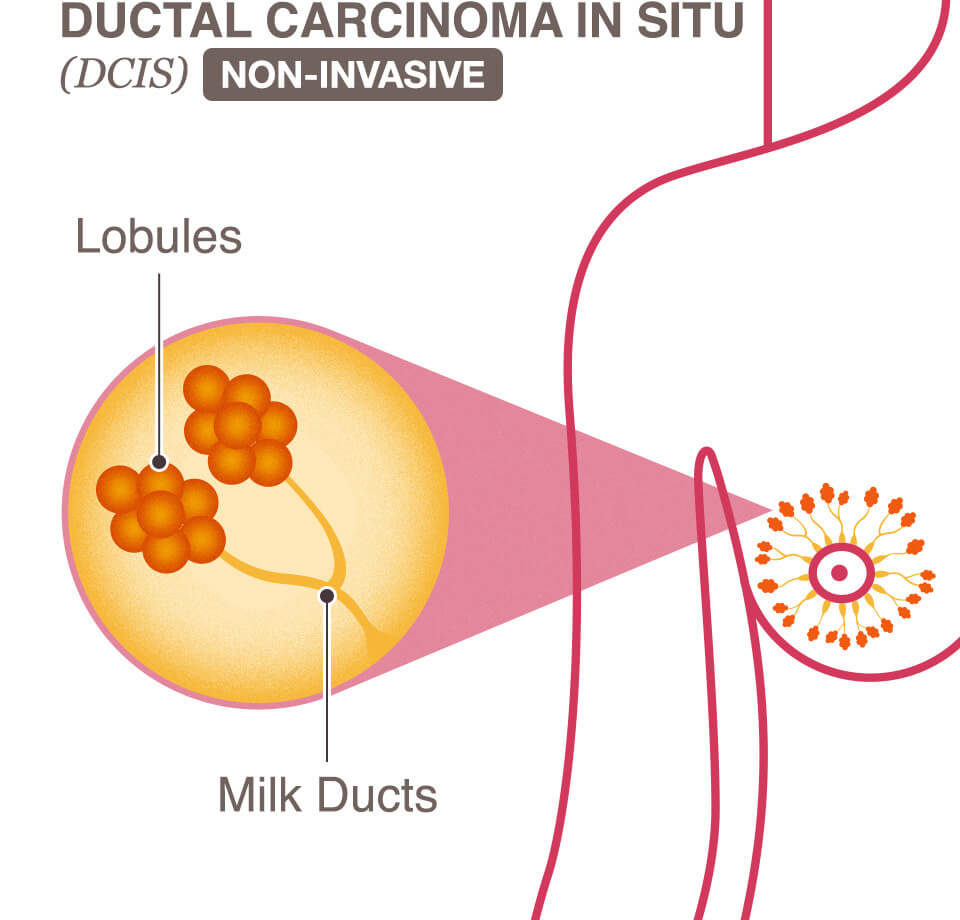
Ductal carcinoma in situ (DCIS) is a common form of breast cancer, accounting for approximately 20-25% of all new breast cancer cases in the United States. DCIS is a non-invasive cancer where abnormal cells have been found in the lining of the breast milk ducts.
Milk ducts are tiny tubes that carry milk from the lobules of the breast to the nipples for breastfeeding. Breast cancer usually begins in the cells of these milk ducts or lobules. DCIS is cancer in the beginning stage before it spreads beyond the milk ducts.
Because the cancerous cells have not spread outside of the milk ducts into the surrounding breast tissue, it means that the cancer is non-invasive and has not invaded (spread to) other tissue in the breast or the lymph nodes.
Ductal carcinoma in situ is also called intraductal carcinoma and is Stage 0 breast cancer. DCIS is early-stage cancer that is highly treatable. Nearly all women with DCIS can be cured. However, if left untreated or undetected, DCIS may spread into the surrounding breast tissue and could become a more advanced cancer. When DCIS spreads beyond the milk ducts and invades other areas of the breast, it becomes invasive ductal carcinoma (IDC). IDC indicates a higher stage of breast cancer and can become life threatening.
DCIS does not usually present with any noticeable signs or symptoms and is often found as a result of an annual screening mammogram, making early detection the key to finding breast cancer in this early stage.
What does the term “in situ” mean?
The earliest stage of cancer is called “carcinoma in situ.” Carcinoma means “cancer” and in situ is Latin for “in the original place.” Together, ductal carcinoma in situ means that the cancer is only in the place it originated (the milk ducts) and has not spread from that original place.
Jump to
Ductal carcinoma in situ grades
Causes & risk factors of DCIS
Signs and symptoms of DCIS
How is DCIS detected?
Diagnosing DCIS
Pathology & prognostic factors of DCIS
Treatment of DCIS
DCIS prognosis
Ductal carcinoma in situ FAQs
DCIS stories of hope
Ductal carcinoma in situ grades
After a needle biopsy, a pathologist will examine the DCIS cells under a microscope in order to give the cancerous cells a grade. Like other types and stages of breast cancer, DCIS will be given a grade between 1 and 3.
Grades of DCIS
| DCIS Grade | Indication |
| Grade 1 | Cancer cells look much like normal breast cells and tend to grow slowly. |
| Grade 2 | Cancer cells look much like normal breast cells and tend to grow at a moderate pace. |
| Grade 3 | Cancer cells look distinctly different from normal breast cells and tend to grow rapidly. Grade 3 presents an increased chance of an invasive breast cancer diagnosis or recurrence in the future. |
Causes and risk factors of ductal carcinoma in situ (DCIS)
Like other types of breast cancer, the exact cause of DCIS is unknown. However, there are risk factors that may increase the chance of developing DCIS as well as other types of breast cancer. Risk factors for breast cancer include genetic risk factors and environmental & lifestyle risk factors.
Genetic risk factors of DCIS
Genetic risk factors are inherited traits a person is born with that cannot be changed. Genetic risk factors for DCIS include:
- Gender: Women are nearly 100 times more likely to develop breast cancer than men.
- Age: The risk of developing DCIS increases with age. DCIS risk is highest in women between the ages of 65 and 69, though it can occur at any age.
- Family history: If a first-degree relative, such as a mother, sister, father, or child, was diagnosed with breast or ovarian cancer, there is a higher risk of developing breast cancer. The risk increases if the first-degree relative was diagnosed before the age of 50.
- Gene mutations: Those who test positive for a BRCA gene mutation or other type of breast cancer gene mutation have an increased risk of developing breast cancer. Approximately 5-10% of breast cancers of any kind are the result of gene mutations and have been linked to many forms of cancer, including DCIS, ovarian cancer, melanoma, pancreatic cancer, and the early-age diagnosis prostate cancer in men. Those carrying a gene mutation as the cause of their breast cancer are commonly diagnosed under the age of 55 and, in the majority of cases, their breast cancer is invasive. Read more about breast cancer genetics.
- Personal health history: A woman’s personal health history may increase her risk of developing breast cancer. Personal health history factors can include:
- Early menstruation: Starting menstruation before age 12
- Pregnancy: Having a baby after age 30 or never being pregnant
- Late menopause: Starting menopause after age 55
- Previous diagnosis of breast cancer
- Dense breast tissue: Having dense breast tissue can make lumps harder to detect and read on a mammogram, leading to an increased risk of breast cancer.
Environmental & lifestyle risk factors for DCIS
Environmental and lifestyle risk factors are typically under a person’s control and can be changed. Environmental and lifestyle risk factors for DCIS include:
- Lack of physical activity: A sedentary lifestyle can increase the risk of breast cancer.
- Obesity: Being overweight or obese can increase the risk of breast cancer, especially for older women.
- Poor diet: A diet low in fruits and vegetables can increase the risk of breast cancer.
- Drinking alcohol or smoking: Drinking and smoking can lead to an increased risk of developing breast and other types of cancer.
- Combined hormone replacement therapy (HRT): Taking combined HRT for more than 5 years can increase the risk of developing breast cancer.
- Radiation to the chest: Having radiation therapy to the chest for treatment of a different type of cancer, occurring before the age of 30, can increase the risk of breast cancer. While radiation is often an unavoidable therapy for certain illnesses, it is still considered an environmental risk factor because it is not an inherited trait.
Signs and symptoms of ductal carcinoma in situ (DCIS)
Because DCIS is early-stage breast cancer (Stage 0), it typically does not have any noticeable signs or symptoms. In rare cases, some people may experience a breast lump or discharge (clear fluid) from the nipple, but the majority of DCIS cases are found through a mammogram.
While it is rare to see or feel noticeable symptoms with DCIS, an exception is in Paget’s disease of the nipple, which may produce noticeable signs and symptoms. Paget’s disease is DCIS located within the nipple. It appears in the form of itchiness and scaliness of the nipple and sometimes the areola (the darker circle of skin around the nipple).
How is DCIS detected?
The early detection of breast cancer is key to successful outcomes. Early detection means finding cancer in its early stages before it has a chance to spread and when it is easiest to treat.
Early detection of DCIS and all types of breast cancer consists of three main steps:
- Breast self-awareness: When a woman is aware of the way her breasts normally look and feel, it is easier to detect when something has changed. All women age 18 and over are encouraged to perform a monthly breast self-exam to check for changes in their breasts and surrounding tissue. Any changes should be reported to a healthcare professional immediately. While most DCIS cases don’t have any noticeable symptoms, such as a lump, it is still important to perform regular breast self-exams.
- Well-woman exam: It is recommended that all women age 18 and over visit their family physician and/or gynecologist once a year for a physical exam that includes a clinical breast exam. At this appointment, the doctor will discuss the breast health screening schedule that is right for you, as well as other screening exams you should have.
- Mammogram: A mammogram is an x-ray of the breast and is a safe way to detect cancerous tumors or other irregularities, often before any symptoms appear. All women age 40 and over should receive a yearly screening mammogram. If you have a family history of breast cancer, you may need to begin mammograms earlier than 40. Discuss your family history with your doctor to determine the mammogram schedule that is best for you.
3 Steps to Early Detection Guide
Read more about the 3 steps to early detection, including breast self-exams, clinical breast exams, and mammograms, in the free 3 Steps to Early Detection Guide.
Download the free guideDiagnosing ductal carcinoma in situ (DCIS)
DCIS is usually discovered through a regular screening mammogram. If the screening mammogram shows an abnormality or irregularity, a diagnostic mammogram is likely to be performed. A diagnostic mammogram is a more in-depth mammogram and is performed if screening mammogram results are suspicious or if there are symptoms of breast cancer present.
Other tests used to diagnose DCIS include:
- Breast ultrasound: This scan produces penetrative sound waves to create a sonogram image that can be used to help diagnose DCIS.
- Breast MRI: This imaging scan is more sensitive than a mammogram or ultrasound and may be used to help diagnose DCIS.
- Breast biopsy: This test removes tissue or fluid from the suspicious area so that it can be studied under a microscope in a lab. A biopsy is used to help diagnose DCIS.
Pathology and prognostic factors of DCIS
Once a biopsy is complete, a specially trained doctor called a pathologist will review the biopsy and create a pathology report that outlines the characteristics of the cancer, called prognostic factors. These factors assist doctors in determining the best way to treat the specific breast cancer.
There are 3 specific prognostic factors that the pathologist looks for to help determine DCIS treatment needs:
- Estrogen receptor status: If estrogen receptors are found in the cancerous cells, the cancer is estrogen receptor-positive (ER+). This means that the hormone estrogen stimulates these specific DCIS cells to grow and multiply. The percentage of the cells that are ER+ are recorded in the pathology report, along with the grade of the DCIS. The higher the percentage or ER+ cells, the more favorable this prognostic factor is. When the cells are ER+, hormonal therapy will be recommended as a key part of treatment for prevention of recurrence.
- Progesterone receptor status: The progesterone receptor is also determined and, if positive (PR+), is also a favorable prognostic factor.
- HER2 receptor status: HER2, or human epidermal growth factor receptor 2, is relatively new in being measured when only DCIS is present. It helps determine if the DCIS cells are aggressive and overproducing the HER2 protein.
Treatment of ductal carcinoma in situ (DCIS)
Common treatments for DCIS include surgery, radiation, and hormonal therapy, or a combination of these. Chemotherapy is not used to treat DCIS.
Surgery
Two types of breast surgeries, lumpectomy or mastectomy, may be used to remove the cancerous cells from the breast.
Lumpectomy
Lumpectomy, also known as breast-conserving surgery, is the most common treatment for DCIS. A lumpectomy removes only the cancerous tissue and a small margin of normal tissue around it, rather than removing all of the breast tissue. Lymph node removal is not usually needed. A lumpectomy for DCIS is often followed by radiation to reduce the chance of the cancer coming back.
Mastectomy
A mastectomy is the surgical removal of the breast and breast issue. While a lumpectomy is now more common to treat DCIS, a mastectomy may be performed if the cancerous cells are widespread, occur in multiple areas of the breast, or a lumpectomy cannot remove the cancer completely. If a mastectomy is performed, a sentinel node biopsy will likely be performed as well to determine if any of the tissue that contains DCIS cells also contains areas of invasive cancer.
A double mastectomy to treat DCIS is rare, but may be discussed with your healthcare team and surgeon. Individuals who carry a breast cancer gene mutation may be advised to also remove the healthy breast because of risk of developing breast cancer there is higher than average. Additionally, some women choose a double mastectomy, also known as a bilateral mastectomy. Women who have a mastectomy for DCIS typically do not require radiation after surgery.
Radiation
Radiation uses high-energy rays to destroy any remaining cancer cells after surgery to treat DCIS. Radiation reduces the chance of the cancer coming back. However, if the cancerous area is small or low-grade, then radiation may not be needed following surgery. Other factors that may be taken into account when radiation is considered is the patient’s age and prognostic factors. Typically, women over age 70 with estrogen receptor-positive (ER+) DCIS do not receive radiation.
Hormonal therapy
Hormonal therapy may be given to women with estrogen receptor-positive (ER+) DCIS after radiation and/or surgery to decrease the risk of recurrence. Drugs, including tamoxifen (for pre-menopausal women) or anastrozole (for post-menopausal women), can be taken as a pill for up to five years post-surgery.
Ductal carcinoma in situ prognosis
The prognosis for DCIS is excellent. More than 99% of patients diagnosed with DCIS will recover and live more than 5 years after their initial diagnosis. The 5-year measurement is used because most patients are not followed beyond 5 years to track survival rates. If all treatments are completed as prescribed, many women live much longer than the 5 years that they are followed for survival rate tracking.
DCIS recurrence
While some patients may experience a recurrence of DCIS, the recurrence rate for DCIS is generally low, around 15%, for patients who received both surgery and radiation as treatment.
Though the risk of recurrence is relatively low, there are risk factors that may increase the likelihood of DCIS recurring, including:
- A large amount of cancer (10 millimeters or more) was removed in the first round of treatment
- The initial cancer was high- or intermediate-grade
- Radiation is not received after surgery
Additionally, women who have had DCIS have a higher risk of developing invasive breast cancer for up to 25 years after the initial DCIS diagnosis. But it is important to remember that every cancer is different and every woman is different. With early detection and thorough treatment, most women diagnosed with DCIS will live a long life.
Ductal carcinoma in situ (DCIS) FAQs
Can DCIS spread?
If left untreated or undetected, DCIS may spread out of the milk ducts and into the surrounding breast tissue. When DCIS spreads beyond the milk ducts and invades other areas of the breast, it becomes invasive ductal carcinoma (IDC) and advances in stage.
Can DCIS come back?
The recurrence rate of DCIS is generally low, around 15%, for patients who received both surgery and radiation as treatment. However, a small number of women will experience a recurrence of DCIS. In about half of breast cancer recurrence after DCIS treatment, the cancer is found to be invasive, such as invasive ductal carcinoma (IDC) or other types of invasive breast cancer.
Can DCIS become invasive breast cancer?
When left undetected or untreated, DCIS cells may continue to grow and spread, eventually becoming invasive breast cancer once the cancerous cells spread out of the milk ducts and into the surrounding breast tissue or beyond.
Research studies are underway to help determine which type of DCIS cells may grow and spread and which ones will likely not. This information will eventually be helpful in determining which patients with only DCIS need treatment and which do not. Current research shows that women who choose to do mastectomy surgery despite having a small area of DCIS in the breast only have a 1% risk of local recurrence of breast cancer (breast cancer returning at or near the site of the original breast cancer).
Is DCIS hereditary?
Not all DCIS or other breast cancers are hereditary. However, a family history of breast cancer is a risk factor for developing DCIS and other types of breast cancer. Genetic mutations passed through the genes from parent to child, such as BRCA gene mutations, can also increase the chances of developing DCIS, though a genetic (hereditary) link is more commonly associated with invasive breast cancers than DCIS.
DCIS stories of hope
No matter the type of breast cancer, NBCF is here to offer help and hope. Read ductal carcinoma in situ stories of hope on the NBCF blog:
A Story Inked in Hope: Abigail’s Journey Through DCIS
Sources:
Cleveland Clinic
American Cancer Society
American Cancer Society
Oncolink
Penn Medicine
Moffitt Cancer Center
Johns Hopkins